91.-ROTURA
LIVER POST-CHOLECYSTECTOMY .
ABOUT TWO FATAL CASES.
Prof.Garfia.A
91.-Leberruptur als Komplikation der Cholezystektomie. Ein Bericht von zwei Todesfälle.
Prof.Garfia.A
91.-HEPATIC RUPTURE AFTER CHOLECYSTECTOMY. REPORT OF TWO FATAL CASES.
Prof. Garfia.A
Introducción
liver rupture is a rare and unusual event that may result from different etiological mechanisms, among which are:
1 .- traumatic ruptures.
occur from a direct blow on the right upper quadrant, a kick, a traffic accident, etc.
traumatic hepatic rupture, secondary a fall to the ground before hitting the edge of a bed, a table, or tub-or down stairs is a highly unlikely event that could be explained by the fact that the abdomen is protected against a fall-front-for the dampening effect of all four limbs, head and chest. The trauma of abdominal organs occur only when the damping effect is nullified by previous trauma or body by a tremendous impact as a result of abuse or precipitation.
In cases of traumatic liver rupture, some authors (Vocke, 2001. Int J Legal Med 114:244-247) saying you should try to establish causal relationships between the morphological pattern of the tear and the type of trauma suffered by the victim. In this context, forensic doctors can do about the situation of an expert opinion whether a particular type of liver damage was the result of a blow, kick or an accidental fall, or violent. The differential diagnosis between liver damage caused accidentally or intentionally, it is especially difficult when both events have taken place peers. The differentiation of liver injury caused by accident, or intentionally, it is very important in forensic pathology, as is the case with head injuries.

Scheme 1 .-
Reprinted, slightly modified, (Vocke, R. 2001. Int J Legal Med 114:244-247. Liver by isolated rupture force impact: the result of a blow, a kick or a fall? ).
The diagram shows, in the author's experience, the location of the liver breaks in different types of falls to the ground:
1 .- Fall to the ground and hit against the edge of the bed or table. Rupture of the right hepatic lobe capsule, about 4mm profundidad.Muerte fulminant pulmonary thromboembolism.
2. -Fall on the right side of abdomen.Golpe on the edge of the tub. Dead on the third day. Rupture of the inferior right lobe of about 14 cm in length.
3. -drop to the ground. Death after 5 days of caída.Fracturas sacks. Ventro-dorsal break right liver lobe, the size of an orange.
4 .- Fall on the right side of the body, after slipping on a rug on the mattress of the cama.Muerte, two hours after the crash. Rib fractures. Rupture of the right hepatic lobe.
The differential diagnosis includes always Iatrogenic hepatic rupture secondary to the application of CPR. The liver rupture secondary to cardiac massage is directed, preferably between right and left lobes, and are vertical.
2 .- The spontaneous liver rupture (nontraumatic).
are very rare and therefore have little authority to be considered in the differential diagnosis.
The spontaneous liver rupture, nontraumatic, have been described in patients with:
a) liver tumors, benign and / or malignant (carcinomatosis Glisson's capsule)
b) cysts.
c) hepatic amyloidosis.
d) Pre-eclampsia and eclampsia.
e) Peliosis hepatica.
f) Obstruction of the portal or hepatic vein thrombosis.
g) disseminated intravascular coagulation.
3 .- iatrogenic liver ruptures that occur during or several days after surgery on the gallbladder.
The two cases of liver failure presented occurred during, or shortly after a cholecystectomy. In both cases death was delayed and was the result of a hemorrhage of liver parenchymal rupture or the production of a hepatic subcapsular hematoma followed by capsule rupture and massive hemoperitoneum.
CASE NO 1
Case description
It was a woman, 40, who entered a private clinic of a dormitory town in the north Spain, scheduled for cholecystectomy intervention.
The patient died on the third postoperative day in the clinic. I have no information on the clinical diagnosis the cause of death.
Surgeon unusual attendance at the funeral, and his intervention with the family of the deceased.
In a surprising way for the family, the husband and those attending the funeral, the surgeon was made in the act of burial, the order to give our condolences to her husband and family. But the surprising fact for all attendees was that, the aforementioned surgeon, perhaps trying to minimize or mitigate his guilt- asked the husband if the deceased could have been beaten. This caused a huge surprise on the husband who reminds the surgeon that "his wife had been admitted to the clinic, since the surgery until his death."
's husband, aghast, took out a legal complaint in the Court of Guard, following which they proceeded to conduct a judicial autopsy.
Autopsy Findings
During the autopsy revealed the following findings:
1.-Five surgical wounds in the chest.
right 2.-Collapsed lung, iatrogenic.
3.-Hepatomegaly with large areas of liver lacerations, some surgical sutures.
4.-Hemoperitoneum.
Cause of death in the autopsy report.
hypovolemic shock due to multiple liver lacerations with severe hemoperitoneum.
HISTOPATHOLOGY
massive hepatic hematoma with rupture capsular and multiple liver lacerations, surgical sutures and bandages and using gauze and hemostatic material.
occur from a direct blow on the right upper quadrant, a kick, a traffic accident, etc.
traumatic hepatic rupture, secondary a fall to the ground before hitting the edge of a bed, a table, or tub-or down stairs is a highly unlikely event that could be explained by the fact that the abdomen is protected against a fall-front-for the dampening effect of all four limbs, head and chest. The trauma of abdominal organs occur only when the damping effect is nullified by previous trauma or body by a tremendous impact as a result of abuse or precipitation.
In cases of traumatic liver rupture, some authors (Vocke, 2001. Int J Legal Med 114:244-247) saying you should try to establish causal relationships between the morphological pattern of the tear and the type of trauma suffered by the victim. In this context, forensic doctors can do about the situation of an expert opinion whether a particular type of liver damage was the result of a blow, kick or an accidental fall, or violent. The differential diagnosis between liver damage caused accidentally or intentionally, it is especially difficult when both events have taken place peers. The differentiation of liver injury caused by accident, or intentionally, it is very important in forensic pathology, as is the case with head injuries.

Scheme 1 .-
Reprinted, slightly modified, (Vocke, R. 2001. Int J Legal Med 114:244-247. Liver by isolated rupture force impact: the result of a blow, a kick or a fall? ).
The diagram shows, in the author's experience, the location of the liver breaks in different types of falls to the ground:
1 .- Fall to the ground and hit against the edge of the bed or table. Rupture of the right hepatic lobe capsule, about 4mm profundidad.Muerte fulminant pulmonary thromboembolism.
2. -Fall on the right side of abdomen.Golpe on the edge of the tub. Dead on the third day. Rupture of the inferior right lobe of about 14 cm in length.
3. -drop to the ground. Death after 5 days of caída.Fracturas sacks. Ventro-dorsal break right liver lobe, the size of an orange.
4 .- Fall on the right side of the body, after slipping on a rug on the mattress of the cama.Muerte, two hours after the crash. Rib fractures. Rupture of the right hepatic lobe.
The differential diagnosis includes always Iatrogenic hepatic rupture secondary to the application of CPR. The liver rupture secondary to cardiac massage is directed, preferably between right and left lobes, and are vertical.
2 .- The spontaneous liver rupture (nontraumatic).
are very rare and therefore have little authority to be considered in the differential diagnosis.
The spontaneous liver rupture, nontraumatic, have been described in patients with:
a) liver tumors, benign and / or malignant (carcinomatosis Glisson's capsule)
b) cysts.
c) hepatic amyloidosis.
d) Pre-eclampsia and eclampsia.
e) Peliosis hepatica.
f) Obstruction of the portal or hepatic vein thrombosis.
g) disseminated intravascular coagulation.
3 .- iatrogenic liver ruptures that occur during or several days after surgery on the gallbladder.
The two cases of liver failure presented occurred during, or shortly after a cholecystectomy. In both cases death was delayed and was the result of a hemorrhage of liver parenchymal rupture or the production of a hepatic subcapsular hematoma followed by capsule rupture and massive hemoperitoneum.
CASE NO 1
Case description
It was a woman, 40, who entered a private clinic of a dormitory town in the north Spain, scheduled for cholecystectomy intervention.
The patient died on the third postoperative day in the clinic. I have no information on the clinical diagnosis the cause of death.
Surgeon unusual attendance at the funeral, and his intervention with the family of the deceased.
In a surprising way for the family, the husband and those attending the funeral, the surgeon was made in the act of burial, the order to give our condolences to her husband and family. But the surprising fact for all attendees was that, the aforementioned surgeon, perhaps trying to minimize or mitigate his guilt- asked the husband if the deceased could have been beaten. This caused a huge surprise on the husband who reminds the surgeon that "his wife had been admitted to the clinic, since the surgery until his death."
's husband, aghast, took out a legal complaint in the Court of Guard, following which they proceeded to conduct a judicial autopsy.
Autopsy Findings
During the autopsy revealed the following findings:
1.-Five surgical wounds in the chest.
right 2.-Collapsed lung, iatrogenic.
3.-Hepatomegaly with large areas of liver lacerations, some surgical sutures.
4.-Hemoperitoneum.
Cause of death in the autopsy report.
hypovolemic shock due to multiple liver lacerations with severe hemoperitoneum.
HISTOPATHOLOGY
massive hepatic hematoma with rupture capsular and multiple liver lacerations, surgical sutures and bandages and using gauze and hemostatic material.
 Case 1
Case 1 Fig.1.-Break impairment "during surgery for cholecystectomy, followed by death delayed the third day after surgery.
Show macroscopic appearance of the right hepatic lobe. There are multiple lacerations and fractures, one of which presents a surgical suture which includes a vision for gauze and bandages used as material hemostático.La patient was sent to the Board under these conditions, suffering a death, delayed by hemorrhagic shock On the third day after surgery. Prof. Garfia.A

Case 1
Fig . 2 .- To show a breakdown of the suture and "made hemostatic technique." The patient was sent to the room where he died, the third day. With regard to the cause of the break I think that a such a scale destruction inflicted during the intervention should have occurred or during laparotomy-induced by separators or surgical-patient drop the operating table with a direct impact on the ground with the open abdomen. The real cause was never known. Prof. Garfia.A

Case 1
Fig. 3 .- Section lobe right liver showing various intraparenchymal hemorrhagic foci.
Prof.Garfia.A 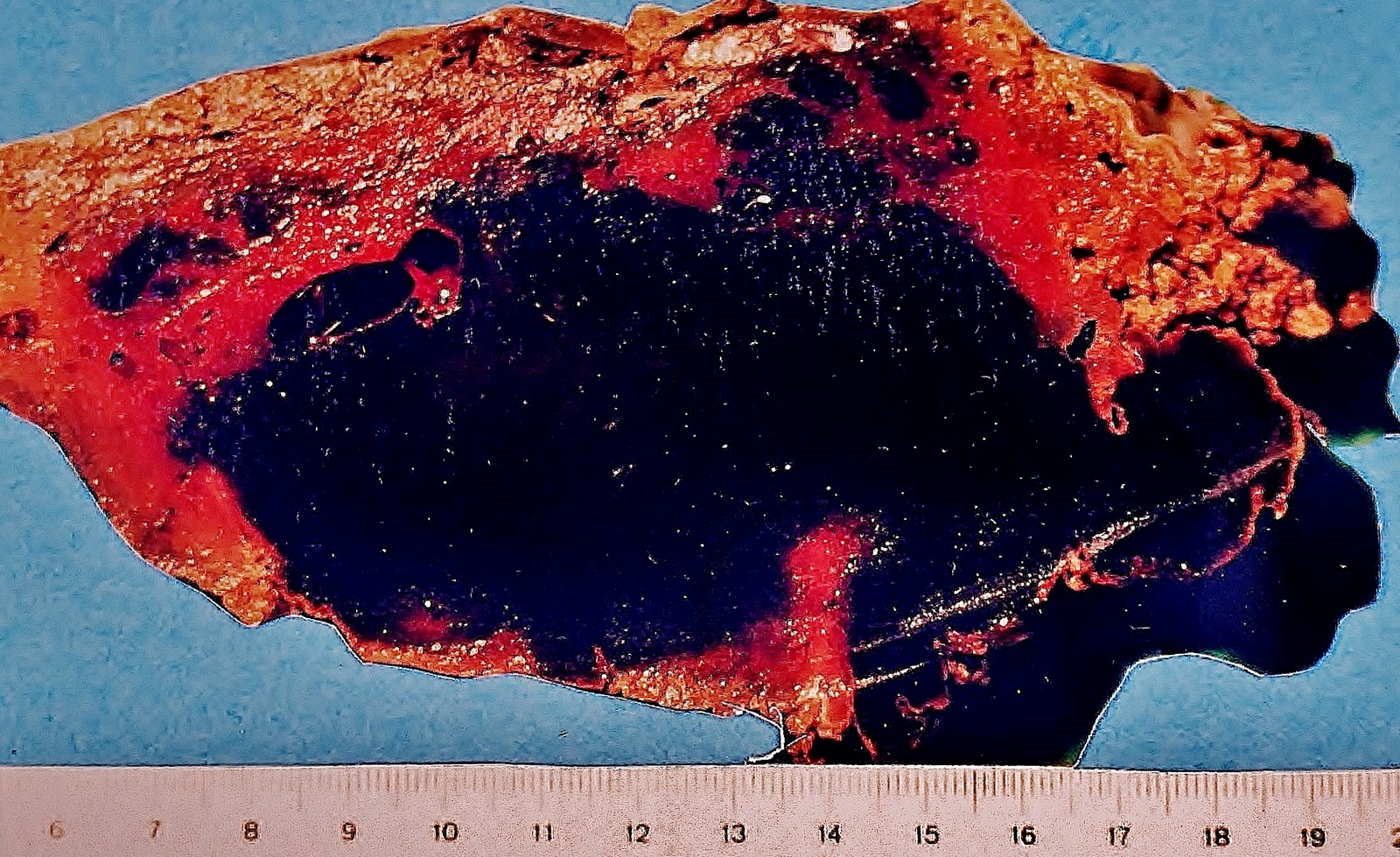
Fig. 4. -Detail of another section of the same lobe as shown here, the coalescence of hemorrhagic foci, resulting in a large hematoma that occupies almost the entire liver parenchyma.
Prof.Garfia.A
Case No. 2
Case description
Personal history ;
This was a patient of 73 years, who had a history of right renal atrophy and left nephrolithiasis.
A few days before hospital admission had pain in hypochondrium and right iliac fossa, which was accompanied by bilious vomiting and fever.
A few days before hospital admission had pain in hypochondrium and right iliac fossa, which was accompanied by bilious vomiting and fever.
current disease
entered a hospital in reference to the object to be studied in the process.
the beginning of his admission he hydronephrosis accompanied of sepsis, which required ureteral catheterization and antibiotic treatment, as well as left percutaneous nephrostomy and ureteral catheterization by the presence of ureteral calculus at the level of L4.
Despite the persistence of sepsis, with fever and leukocytosis, cause renal, surgery is indicated cholecystectomy - operation that was considered high-risk after the diagnosis of acute cholecystitis. Immediate surgical treatment was decided.
During surgery, the surgeons described the existence of a Acute gangrenous cholecystitis with the presence of large stones.
was performed a cholecystectomy, from bottom to neck, the difficulty encountered in making proper anatomical dissection of the pedicle.
The excised gallbladder was informed by the Hospital Pathology Service, as gall affects acute necrotizing cholecystitis.
Postoperative
After intervention, fever disappeared and there was a slight improvement of general condition.
Al third postoperative day with increasing pain in the right upper quadrant, which prompted the administration of various analgesic drugs (Paracetemol, dolantina and Nolotil).
That same night, the patient died suddenly.
AUTOPSY FINDINGS
1.-External Review
Corpse woman, 73 years, obese, which presents catheterization and catheter. There is an laparotomy scar, about 19 cm, closed with staples, has a drain bloody fluid that comes out.
The body has pale skin and discreetly marked edema of the extremities.
2.-Internal review
2.1.-Head
Without interés.Encéfalo congestive .
Thorax .- 2.2.-
bilateral pleural effusion, Aspect serous, in an amount of 400 ml. Pale and edematous lungs (970 g, both). Abundant white foam in the trachea and bronchi. Heart without significant changes.
2.3.-Abdomen
hemoperitoneum of about 100 ml.
Rich clots right iliac fossa.
Hematoma subcapsular liver that affects two-thirds of them with parenchymal destruction.
right kidney, atrophic. Bruised left kidney cortical, which grows to about 4 cm in diameter.
Cause of death in the autopsy report
Acute liver failure.
entered a hospital in reference to the object to be studied in the process.
the beginning of his admission he hydronephrosis accompanied of sepsis, which required ureteral catheterization and antibiotic treatment, as well as left percutaneous nephrostomy and ureteral catheterization by the presence of ureteral calculus at the level of L4.
Despite the persistence of sepsis, with fever and leukocytosis, cause renal, surgery is indicated cholecystectomy - operation that was considered high-risk after the diagnosis of acute cholecystitis. Immediate surgical treatment was decided.
During surgery, the surgeons described the existence of a Acute gangrenous cholecystitis with the presence of large stones.
was performed a cholecystectomy, from bottom to neck, the difficulty encountered in making proper anatomical dissection of the pedicle.
The excised gallbladder was informed by the Hospital Pathology Service, as gall affects acute necrotizing cholecystitis.
Postoperative
After intervention, fever disappeared and there was a slight improvement of general condition.
Al third postoperative day with increasing pain in the right upper quadrant, which prompted the administration of various analgesic drugs (Paracetemol, dolantina and Nolotil).
That same night, the patient died suddenly.
AUTOPSY FINDINGS
1.-External Review
Corpse woman, 73 years, obese, which presents catheterization and catheter. There is an laparotomy scar, about 19 cm, closed with staples, has a drain bloody fluid that comes out.
The body has pale skin and discreetly marked edema of the extremities.
2.-Internal review
2.1.-Head
Without interés.Encéfalo congestive .
Thorax .- 2.2.-
bilateral pleural effusion, Aspect serous, in an amount of 400 ml. Pale and edematous lungs (970 g, both). Abundant white foam in the trachea and bronchi. Heart without significant changes.
2.3.-Abdomen
hemoperitoneum of about 100 ml.
Rich clots right iliac fossa.
Hematoma subcapsular liver that affects two-thirds of them with parenchymal destruction.
right kidney, atrophic. Bruised left kidney cortical, which grows to about 4 cm in diameter.
Cause of death in the autopsy report
Acute liver failure.
Histopathology
were issued the following diagnoses:
.- 1.-Heart
slight cardiomegaly right ventricular hypertrophy (0.7-0.8 cm).
2.-Lung .-
extensive congestion and alveolar edema. Morphological signs of shock. Leukostasis.
3.-Liver .-
massive hepatic hemorrhage right hepatic lobe. Subcapsular hematoma. Rupture of Glisson's capsule. Bed surgical removal of the gallbladder and granulation tissue, young, at the surgical site.
left kidney .-
exacerbated chronic pyelonephritis. Exacerbations of chronic Perinefritis.Ureteritis. Hemorrhagic necrosis of the renal papillae. subcapsular hematoma measuring 3x3 cm in diameter, being organized.

Case 2
Fig. 1 .- Liver. Upper face. presents multiple breaks Glisson's capsule with capsular dissection parenchymal tears at several points. Death on the third day of intervention cholecystectomy. Prof. Garfia.A

Case 2
Fig. 2 .- Hígado.Lóbulo right liver. Underside. Shown large subcapsular hematoma and capsular rupture and folding the left side, suggesting that the bruising had started on the left side of the right hepatic lobe.
The pathophysiology of subcapsular hematoma formation seems to depend, according to some authors, of a mechanical problem with obstruction to blood flow out within the liver parenchyma. Normal arterial blood supply to coexist with an obstruction to venous return, lead to an increase of intrahepatic blood pressure, followed by rupture and hemorrhage. I think that we can not rule out a vascular rupture of the hepatic hilum, with escape of blood into the subcapsular space during surgery.
Prof.Garfia.A

Case 2 .-
left kidney.
Showing hemorrhagic necrosis of the renal papillae and subcapsular hematoma (left percutaneous nephrostomy), who was being organized by granulation tissue. Note extreme pallor of the renal parenchyma. Death was caused by hemorrhagic shock. In the lungs, circulating megakaryocytes were numerous (morphological signs of shock).
0 comments:
Post a Comment